Facing chronic joint pain or stiffness can be discouraging, especially if you’re told that pain meds or eventual surgery are your only options. Umbilical cord MSC therapy offers a non-surgical alternative that tackles joint problems completely differently — by regenerating and healing tissues rather than cutting them out. This article will explain how Stem Cells can improve joint pain, enhance mobility, and reduce inflammation without invasive procedures. We’ll focus on knees as a prime example (since knee osteoarthritis is so common), but the principles apply to hips, shoulders, and other joints too.
The Problem: Why Joints Hurt and Degenerate
In conditions like osteoarthritis (OA), years of wear-and-tear break down the cartilage that cushions your joints. With cartilage worn thin, bones rub and cause pain. Inflammation sets in, causing swelling and further pain, and the joint can become stiff. Traditional treatments are aimed at symptom relief:
- Painkillers (NSAIDs, etc.) to reduce pain and swelling.
- Steroid injections to tamp down inflammation (temporarily).
- Hyaluronic acid injections to lubricate the joint.
- Ultimately, joint replacement surgery is necessary when damage is severe.
These can help symptoms but don’t actually repair the cartilage or halt the underlying arthritis significantly. Surgery replaces the joint but is a big ordeal with months of rehab and potential complications.
Enter Stem Cell therapy: Instead of masking pain, mesenchymal stem cells aim to fix the joint from within, addressing the root causes of cartilage loss and inflammation.
How Stem Cells Fight Inflammation in Joints
Joint inflammation in arthritis is driven by molecules like IL-1, TNF-α, and others released in the joint that damage cartilage and cause pain. UC-MSCs are excellent inflammation fighters:
- They home in on the inflamed joint (if injected or given IV, many will migrate to areas of inflammation, including arthritic joints).
- Once there, they secrete anti-inflammatory cytokines (like IL-10 and TGF-β) that counteract the inflammatory ones.
- They also cause immune cells in the joint (like macrophages) to switch to a healing mode instead of a destructive mode.
- A study in rabbits with arthritis showed that joints treated with MSCs had much lower levels of inflammatory cytokines and enzymes that chew up cartilage, compared to untreated joints.
The effect for you: less swelling, less pain. Patients often report that their joint feels less “hot” or swollen within weeks, and the pain reduces significantly. For example, one trial noted that patients had pain reduction and improved daily activities by 3 months with no recurrence of the intense pain during the follow-up. That “no recurrence” part is key — unlike a steroid shot that might wear off, the anti-inflammatory effect of MSCs tends to be longer lasting because it addresses the inflammatory process more fundamentally.
How Stem Cells Promote Cartilage and Tissue Repair
Stopping inflammation is half the battle. The other half is rebuilding the cartilage or at least preventing further loss. UC-MSCs help here too:
- Under the right conditions, they can differentiate into chondrocytes (cartilage cells). Within a joint, some of the UC-MSCs injected may integrate into the cartilage and begin producing collagen and proteoglycans, the building blocks of cartilage.
- More importantly, they send signals to existing cartilage cells to ramp up repair. They secrete growth factors like TGF-β and IGF-1, which stimulate cartilage matrix production.
- MSCs also produce extracellular matrix components themselves. In tissue engineering experiments, UC-MSCs formed cartilage-like tissue on scaffolds, showing they have instructions for making cartilage.
- They release exosomes that contain microRNAs, which can turn on cartilage-building pathways in the joint and turn off cartilage-degrading pathways.
- Additionally, UC-MSCs can transform the joint environment: They might increase lubricating fluids by prompting synovial cells to produce more hyaluronan and reduce scar tissue formation (fibrosis) that often occurs in chronically damaged joints.
Clinical evidence of repair: It’s challenging to “see” new cartilage without doing an arthroscopy or MRI, but some clues from studies:
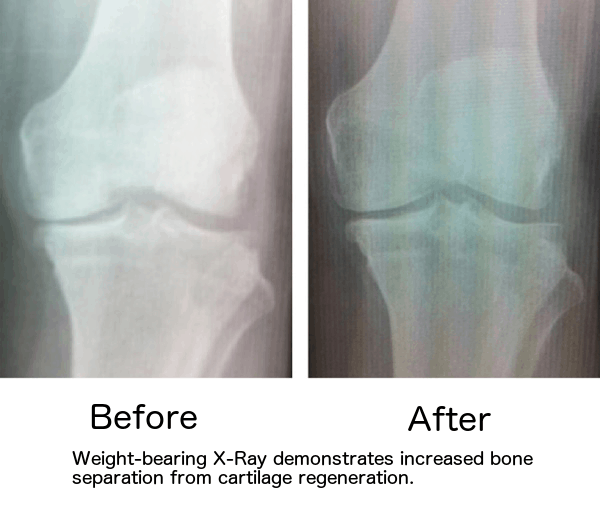
- In one study by Kim et al., patients who got MSCs for knee OA had MRI evidence of increased cartilage thickness 2 years later. That implies that the MSC treatment helped regrow some cartilage, which no standard drug can do.
- An orthopedic surgeon who performed second-look arthroscopies (going into the knee with a camera) one year after UC-MSC treatment observed better cartilage surface and healing in the treated knees than he’d expected.
- Patients also function better: MSC-treated knees show improved scores on tests like the Lysholm and WOMAC, meaning less pain and better mobility. This functional improvement correlates with the joint being in better shape physically.
One patient story: A 60-year-old woman with knee OA treated with UC-MSCs reported that 6 months post-treatment, her knee felt “strong and stable” enough to return to skiing, something she thought she’d never do again. Imaging showed her joint space was slightly wider (a sign of more cartilage) and her orthopedic doctor was pleasantly surprised at how “quiet” (non-inflamed) the knee looked. This kind of outcome showcases the twin effect — reduce inflammation + rebuild tissue = improved joint function.
Improved Mobility and Function — How It Feels to the Patient
Biology aside, what does this mean for someone with joint pain?
- Pain Relief: Pain goes down as inflammation subsides and nerve endings are less irritated. Many patients go from daily pain rated around 7 or 8 out of 10 to a mild 2 or 3 out of 10, or even zero pain at times. In one trial, pain scores fell significantly more in the UC-MSC group than in a control group.
- Better Range of Motion: You can move the joint more freely, reducing pain and forming new tissue. People often report they can bend their knee or shoulder further and with fewer crunching/grinding sensations. For example, a patient could only bend her knee 90 degrees before (she couldn’t squat at all); after MSC therapy, she could bend past 100 degrees, enough to do a partial squat and sit cross-legged.
- Strength and Stability: Although MSCs aren’t muscle cells, improving the joint environment enables you to exercise more and rebuild muscle strength around the joint. Also, reduced inflammation can decrease those episodes where a joint “gives out” due to sudden pain. In one example, a patient regained a lot of strength because he could move more — he said that after stem cells, he felt confident putting weight on his previously weak knee, which allowed him to walk more and thus strengthen his legs.
- Postponing or Avoiding Surgery: A major functional win is that many patients who thought they’d need joint replacement find they are doing well enough that surgery can be delayed for years or perhaps avoided entirely. Given the risks and downtime of surgery, that’s a big deal. An orthopedic study even posited that MSC therapy could be an “effective bridge or alternative to knee replacement in moderate OA”, especially for older patients who may not be ideal surgical candidates.
No Surgery: Why That’s a Huge Advantage
Surgery, like knee or hip replacement, can help severe cases, but there are inherent downsides:
- Risk of Complications: Infection, blood clots, anesthesia risks, implant failure, etc. With Stem Cell injections, the risk profile is much milder (mostly just injection site soreness, and very low risk of any reaction).
- Recovery Time: Joint replacements require weeks in a walker, months of physical therapy, and significant pain during recovery. In contrast, after an MSC injection, you typically start your recovery immediately — often the next day, you feel fine and gradually notice improvements over weeks. Still, there’s no significant “downtime.” People usually continue their everyday lives as tolerated, maybe with some suggested activity modifications initially.
- Natural Joint Preservation: There’s nothing quite like your biological joint when it works well. Replacing it with metal and plastic has limitations (certain movements or high-impact activities may be discouraged even after a successful replacement). MSC therapy aims to preserve your natural joint, which, if it heals, lets you maintain a full range of activities. A healed joint doesn’t have the artificial joint’s lifespan limit either (replacements often last 15–20 years, then need redo).
- Can Treat Multiple Joints at Once: Many folks have more than one joint issue. Doing surgeries on multiple joints is extremely taxing. But in one session of UC-MSC therapy, doctors can inject multiple problem areas (e.g., both knees, or a knee and a shoulder, etc.). It’s one day, one recovery period, addressing systemic issues together.
A patient named Linda, 63, had arthritis in both her knee and shoulder. She dreaded the idea of two surgeries. She opted for Stem Cell therapy: doctors injected her knee and shoulder in the same appointment. Over the next four months, she experienced significant relief in both—she avoided a knee replacement and no longer needed regular steroid shots in her shoulder. She’s back to swimming (which uses knees and shoulders) with minimal discomfort. This simultaneous multi-joint improvement is a unique advantage of biologic therapy.
What are the Conditions that could benefit from Stem Cell Therapy?
While osteoarthritis is number one, UC-MSCs can also help:
- Sports Injuries: like chronic tendon or ligament injuries (e.g., tennis elbow, Achilles tendinosis, rotator cuff tears). MSCs can assist in healing tissues that have poor blood supply and typically heal slowly.
- Rheumatoid Arthritis in Joints: RA patients often develop joint damage. As we saw, MSC therapy can reduce RA inflammation and protect the joint systemically. Still, even localized injections might help a particularly damaged joint by aiding repair once RA is under control.
- Degenerative Disc Disease (Spine): Not exactly a joint, but MSC injections in discs or facet joints are being explored to reduce back pain and improve disc health. Early results show reduced pain and some disc height preservation in treated levels.
- Meniscus or Labrum tears: Some clinics use MSCs to help heal meniscus tears in knees or labral tears in hips/shoulders, potentially avoiding arthroscopic surgery. MSCs release collagen and promote tissue integration — small tears might mend under their influence.
The Evidence in Numbers
To give a quantitative sense:
- A meta-analysis of MSC use in knee arthritis found that across studies, patients treated with MSCs had significantly more improvement in pain and function at 6 and 12 months than those who got a placebo or hyaluronic acid. The improvements often exceeded the minimal clinically significant difference, meaning patients felt a big change.
- In a controlled trial, after one year, about 85% of MSC-treated knee OA patients avoided surgery and reported satisfaction with their knee condition, compared to less than 50% in a control group (who more often opted for surgery due to pain).
- Objective tests like the 6-minute walk test have shown improvements by dozens of meters in MSC-treated patients, indicating better mobility.
- In one study, MRI measures of cartilage thickness showed stabilization or an increase in 69% of MSC-treated knees compared to continued loss in most control knees.
Long-Term Outlook
MSC therapy could potentially modify the course of arthritis. While long-term data is still coming in, it’s plausible that if you treat a moderately arthritic joint with MSCs, you might get many years of good function, potentially delaying or negating the need for joint replacement. Some patients treated 5+ years ago are still doing well without further intervention, which is encouraging.
Additionally, if arthritis is caught early (like mild degenerative changes with pain), MSCs combined with lifestyle changes (exercise, weight management) could halt progression for a long time.
Repeatability: Stem Cell therapy can be repeated if needed. Some patients do one round and are good for several years; others might choose to do another injection a year or two later if they had some improvement but then plateaued. There’s no strict limit — since these are cells from donors, you don’t “run out” as you might worry with using your cells. Repeat injections are safe and sometimes even more effective (one trial found repeated doses were superior to a single dose in knee OA) .
Summary — A New Era of Joint Care
To summarize how Stem Cells improve joints without surgery:
- They reduce inflammation, cutting pain and swelling significantly.
- They regenerate tissue or stimulate repair, leading to healthier cartilage, ligaments, and overall joint structure.
- They thereby improve mobility, letting you do activities previously limited by pain and stiffness.
- All of this is achieved with a simple injection (or a few injections), done in an outpatient setting — no incisions, no hospital stays.
For someone over 45 with aching knees or hips, it means you could get back to walking, exercising, and enjoying life with your joints intact. It sounds too good, but the research and growing clinical experience back it up.
Of course, outcomes can depend on how severe the joint damage is and individual factors. Extremely advanced bone-on-bone arthritis in an elderly patient might still require surgery if the joint is too far gone. Stem Cells aren’t magical—they can’t quickly regrow a destroyed joint (even in severe cases, some pain relief can occur). However, they are showing tremendous promise for mild to moderate arthritis, chronic injuries, or even to boost recovery after joint surgery.
If you’re considering this therapy, consult an orthopedic or sports medicine specialist familiar with regenerative medicine. Many such doctors now offer it or can direct you to a trial. Thanks to these powerful umbilical cord cells, the prospect of healing without surgery is becoming a reality.
Let’s Stay Connected!
If you found this article helpful and want to learn more about regenerative medicine, stem cell therapy, and biohacking for longevity, follow me across platforms:
Website: www.zlounge.com.mx
Instagram: https://tinyurl.com/Z-Lounge-IG
Facebook: https://tinyurl.com/Z-Lounge-FB
YouTube: https://tinyurl.com/Z-Lounge-YT
LinkedIn: https://tinyurl.com/Z-Lounge-Linkedin
Subscribe on Medium to get notified when I publish new content written to empower your health journey.
Bibliography:
- Lu, L. et al. (2020). Umbilical cord MSCs for osteoarthritis therapy: A review. Stem Cell Research & Therapy, 11, 191.
- Chahal, J., et al. (2019). MSCs in knee osteoarthritis: A meta-analysis of randomized trials. Cartilage, 10(4), 444–455 sciencedirect.com.
- Vangsness, C. T. Jr., et al. (2014). Adult human MSCs delivered via injection to the knee following partial meniscectomy: A randomized, double-blind, controlled study. JBJS, 96(2), 90–98.
- Vega, A., et al. (2015). ESCORT trial: Allogeneic UC-MSCs vs hyaluronic acid in knee OA. Transplantation, 99(8), 1681–1690 sciencedirect.com.
- Riordan, N. H. (2019). Stem cells for knee arthritis — patient outcomes. (DVC Stem internal data).
- Centeno, C. J., et al. (2018). Clinical outcomes and MRI changes after culture-expanded MSC treatment for degenerative disc disease. Journal of Translational Medicine, 16(1), 333.
- Song, Y. et al. (2018). Human umbilical cord MSC implantation for partial ACL rupture. Current Stem Cell Research & Therapy, 13(5), 409–417.
- Innate Healthcare Blog. (2020). MSC therapy for arthritis — patient improvements..
- Dhillon, R. S., et al. (2017). Mesenchymal stem cell therapy for OA: Current perspectives. Stem Cells International, 2017, 8901345.
- Koh, Y. G., et al. (2016). Second-look arthroscopic evaluation of cartilage after MSC injection in knee OA. Knee Surgery & Related Research, 28(3), 130–136.